


For Stronger FOOThold
Enjoying this exclusive issue on foot n ankle

Navigation? Check!
Navigation, as a technology, was a logical step in the evolution of joint arthroplasty. Although it is more than a decade old in knees, it paved the way for the current generation of Robotics.
Although the current generation of Ankle arthroplasty implants has improved survivorship, the management of deformities plays a key role in longevity. One important factor is the placement of cuts and Exatech have achieved the next logical step in evolution.

GPS Ankle (DOGE has taken off the creativity fund I suppose)
‘GPS ankle’ touted as the world’s first Navigation system for ankle arthroplasty, the system allows everything you expect from a standard Navigation. Resection height, angle, intra-op implant size planning and pre- and post-op joint Kinematics measurement.

Preclinical studies (bench testing and sawbones) show accuracy close to 2mm and 2 degrees relative to the surgical plan. However, we haven’t been able to verify this claim as the quoted papers are not to be found. There is no literature yet to suggest Navigation is superior but steps like these will enable us to move on to Robotics next.
But is Robotic joint replacement any better? We let you decide.
Be not only a good Clinician but also a great showman!
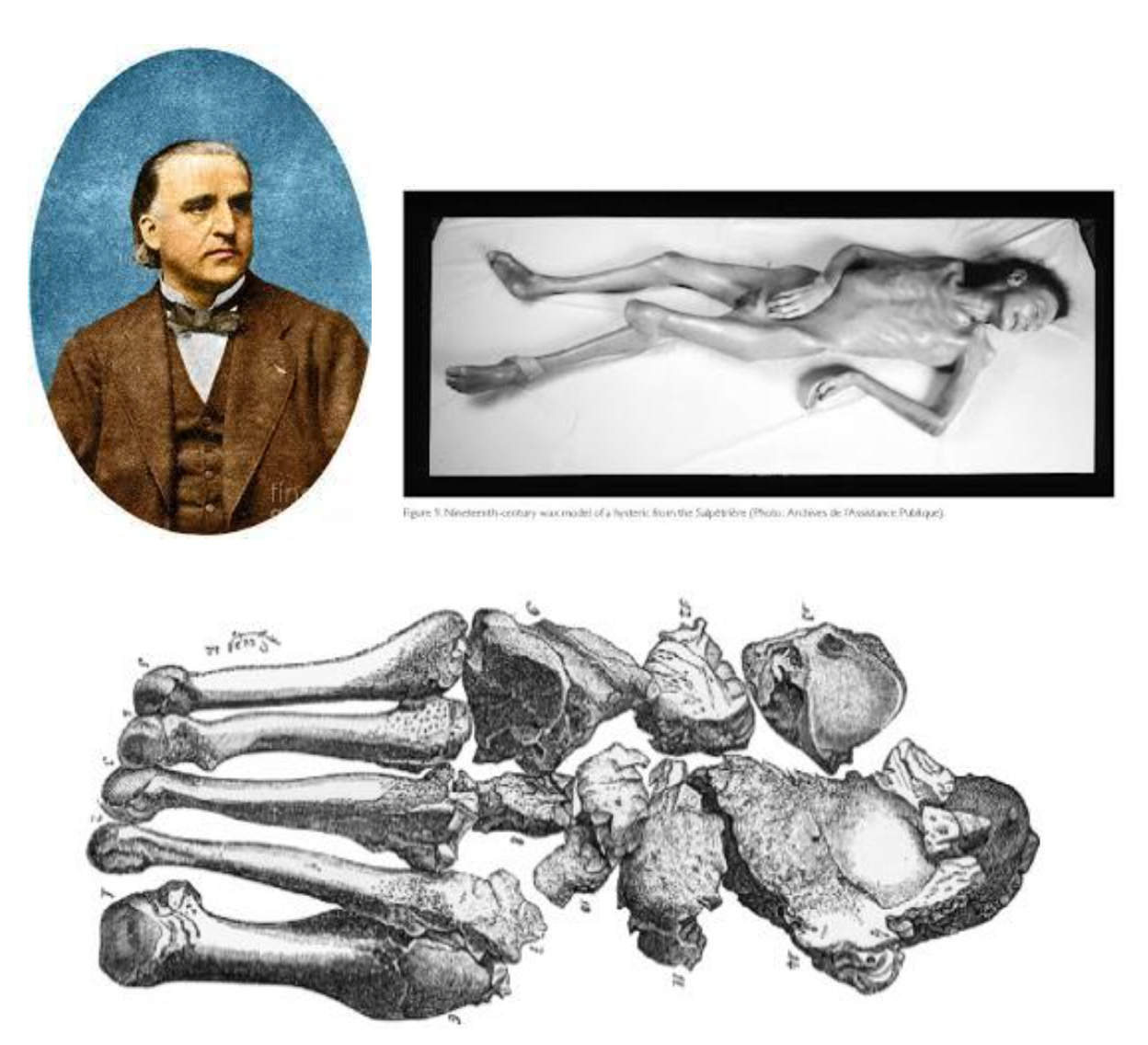
Charcot’s foot—named after the French surgeon Jean-Martin Charcot—is probably one of his most famous discoveries. Back in the day, he was working at the Salpêtrière hospital in Paris, which mainly treated the poor. As a neurologist and rheumatologist, he was the first to describe joint problems linked to Tabes dorsalis (a complication of neurosyphilis), which was then called progressive locomotor ataxia. But like many doctors of his time, he believed most neurological disorders were hereditary—after all, germ theory was still in its early days!
Most surgeons just assumed that the changes in the feet of ataxic patients were caused by ataxia itself. But he was a sharp clinician and noticed what others had missed – the bone and joint changes started before the well-known motor incoordination and locomotor ataxia. He described how the heads of bones wore down, ligaments became extremely loose, and subluxations were common. He even pointed out that while sensations like touch, pressure and temperature were reduced but not completely abolished! Now think how keen observational skills were!
Charcot wasn’t just a brilliant doctor; he was also a bit of a showman. His medical demonstrations were legendary, drawing crowds that included not only students and doctors but also regular folks just curious to see the spectacle.
One of his most famous "performances" took place in 1881 at the 7th International Medical Congress in London. Picture this: a room full of medical legends like Joseph Lister, Louis Pasteur, Robert Koch, and Rudolf Virchow, all watching as Charcot put on a show. He even brought a life-size wax model of a 60-year-old woman named Berthelot—complete with her entire skeleton who had Charcot’s foot! He showcased her disease progress with various clinical photographs as well. His presentation was so detailed and visually impressive that it was the 19th-century version of a multimedia experience. Sir James Paget, another big name in medicine, was so impressed that he declared, "This … a distinct pathological entity, deserves the name by which it will be known—Charcot’s disease."
Pretty cool, right? Charcot was more than just a doctor—he was a pioneer who knew how to make science interesting!
TENDINS-A – Hot Tool in the box that’s worth a try !!
Achilles tendinopathy is a common condition in foot and ankle clinics, however, no specific patient-reported outcome measures (PROMs) are commonly used in clinical practice. This may be due to the concern that the existing PROMs such as Foot and Ankle Outcome Score (FAOS) or Victorian Institute of Sport Assessment–Achilles (VISA-A) have insufficient content and structural validity specific to the condition. However, the new Tendinopathy Severity Assessment –Achilles (TENDINS-A) appears to have sufficient content validity, construct validity, and test-retest reliability.
The TENDINS-A was co-designed by people with Achilles tendinopathy, expert clinicians, and researchers to evaluate the level of disability that results from the condition. The TENDINS-A consists of 13 questions that address the subdomains of disability—Pain, Symptoms, and Function—yielding a total score out of 100, whereby a higher score indicates a higher level of disability. It is available for free.

Simple ways to manage your OCDs - #SurgicalPearl
Check out this simple technique of Torres et al. to manage talar OCDs
1. The patient is put prone, with the ankle hanging freely over the table edge.
2. Standard posterior endoscopic portals (van Dijk technique) are used, with an extra posterolateral portal (1 cm proximal).
3. A 3.5-mm shaver clears fatty tissue and the subtalar joint capsule, exposing the flexor hallucis longus tendon.
4. A 1.2-mm K-wire is inserted through the posterolateral talus under fluoroscopy. It’s over-reamed with an 8-mm cannulated reamer, avoiding cartilage damage.
5. The arthroscope enters the tunnel to visualize necrotic bone. The lesion is cleaned with a curette, spoon, or mini-shaver, keeping the cartilage intact.
6. Bone Graft Harvesting: A cylindrical cancellous bone graft is taken from the distal tibia via the posteromedial portal using a trephine.
7. Bone Graft Placement: The bone plug is inserted through the posterolateral portal into the talar defect and tapped press-fit under the chondral layer.
Simple. Clean. Effective. 💡
Check out the video of the technique here.

Should you walk on your operated ankle sooner?
Ankle fractures are pretty common, and the usual advice after surgery is to avoid putting weight on the leg for about six weeks. But what if patients could start walking earlier—say, just two weeks after surgery? Would it be safe, and could it even help recovery?
The WAX Trial, a randomized controlled study across 23 hospitals in the UK, tested this by comparing early (2 weeks) vs. delayed (6 weeks) weight-bearing in 561 patients who had any surgery for unstable ankle fractures other than nailing. The goal was to see if early weight-bearing was at least as good as (non-inferior to) the standard delayed approach.
After 4 months, patients who started walking earlier had slightly better ankle function scores (OMAS: 65.9 vs. 61.2), though the difference was small. Complication rates were similar (16% early vs. 14% delayed). Plus, early weight-bearing was more cost-effective, saving money for both patients and the healthcare system.
Bottom line? Walking sooner doesn’t cause more harm, might help recovery a bit, and is likely the better option overall. This study gives surgeons the confidence to tell patients: “You don’t have to wait—start walking!” 🚶♂️💪

Answer to the last month question:
Which nerve block provides effective pain control after TKA?
Continuous adductor canal block
Genicular nerve block
Infiltration between the popliteal artery and capsule
A combination of these
A combination of continuous adductor canal block with either genicular nerve block or Infiltration between popliteal artery and capsule is better in TKA pain management according to a network meta-analysis by Wang et al. including 30 studies
Events to check out:
42nd Annual San Diego Course: Arthroplasty, Arthroscopy and Fractures 11 – 13 June 2025, Coronado, USA
Minnesota Anatomic Complex Knee International Symposium (MACKIS) 28-30 May 2025, Eagan, USA
Knee 3600 12 – 13 July 2025 Lima, Peru
Question of the month:
What is the best treatment method for syndesmotic ankle injuries?
Dynamic fixation
Static screw fixation
fibular nails
Any of the above
Wait for our next issue to know the correct answer.
Have a marvellous March guys.