


Hippie love to start the new year
It is a new year. It is also the time to refresh hip updates.

What if…? #NeoArmory:
‘What if’ breaks the Marvel’s mould of superheroes and does a 180 in the storyline, the best one being T’challa’s Quill. Was he any better? That's for you to decide. (We won’t bias your idea) That’s exactly how we felt at today’s Neo-armory section.

Hip Innovation technology, a Georgia (the US one) based venture, has done a ‘what if’ episode. We introduce to you, the brainchild of Dr Termanini, their take on reinventing THR prosthesis.

The Reverse Hip Replacement System
A Cobalt Chrome ball inside the Acetabular cup which articulates with a poly liner attached to the stem. They claim, this design maintains stability with extended Hip ROM, lowers chance of dislocation, reduces contact stresses and minimizes edge loading.
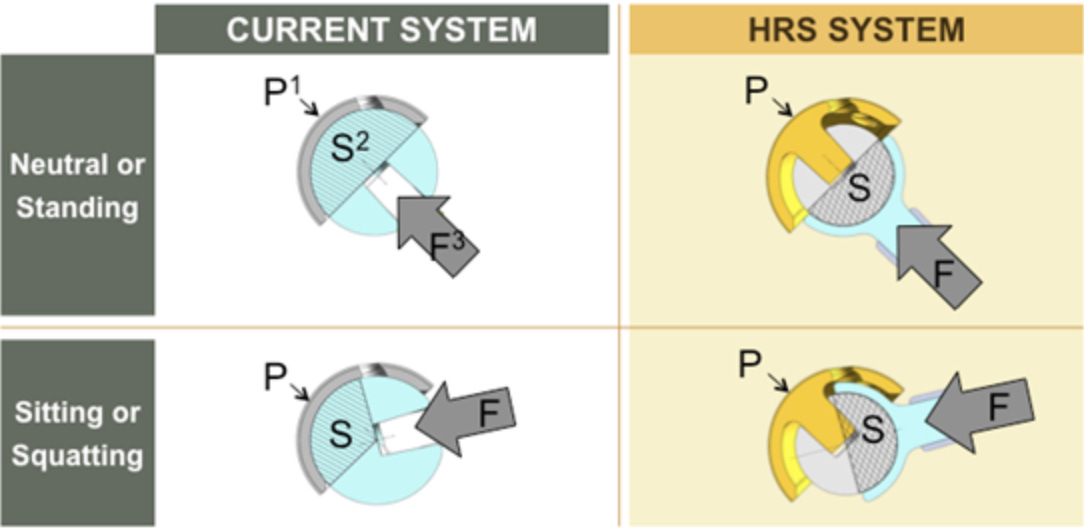
This study shows excellent PROMs data in a 2 year follow up period in 23 patients. We, at the Brewery, are still debating on where to file this? ‘Lesson learnt’ or ‘historical milestone’. What do you think?
Did we steal one of their machine tools? #FromTheHistory:
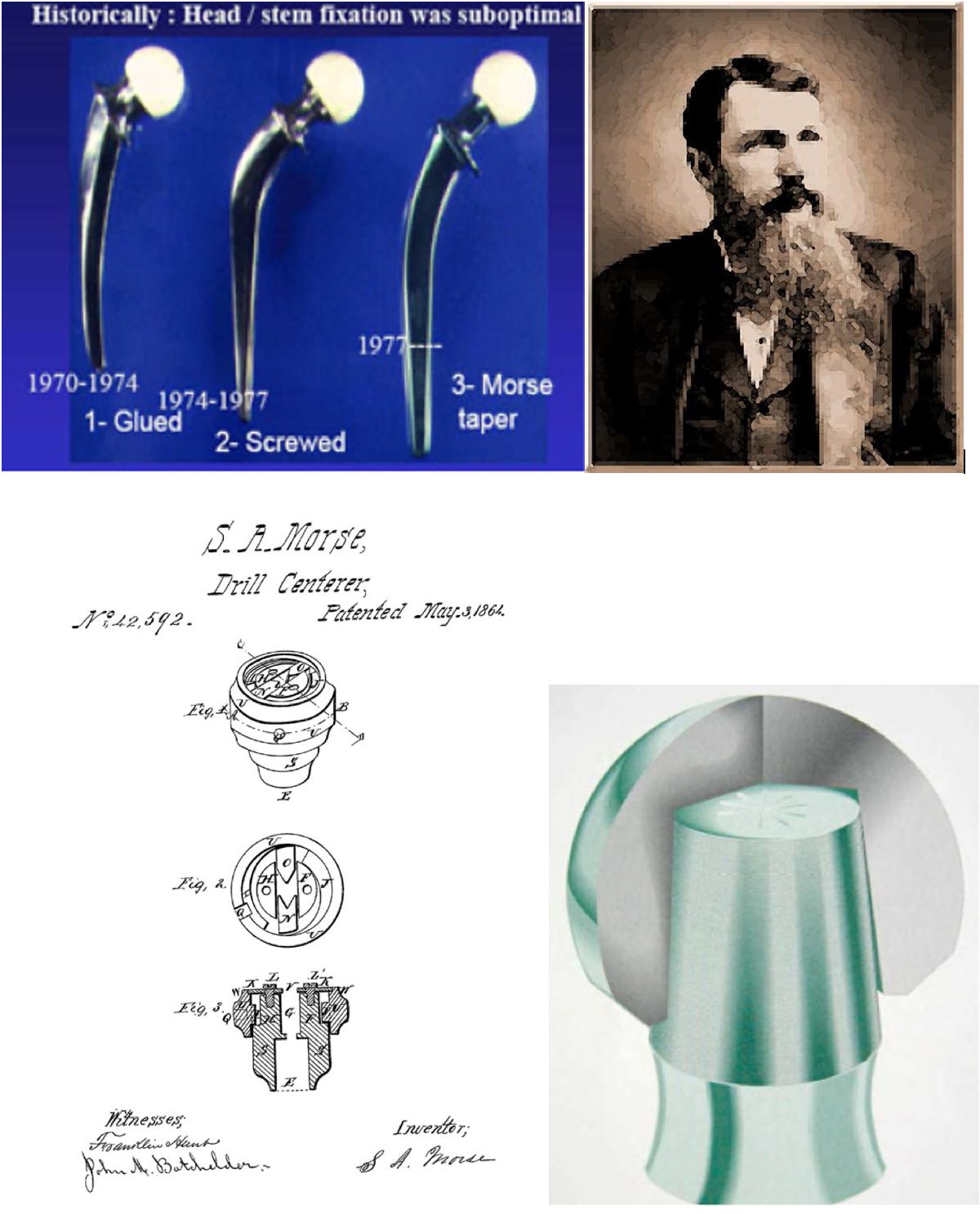
Did you know that Morse taper that is ubiquitous now in total hip replacement was actually designed to be used in machine tools, that too around a century and a half ago! Stephen A. Morse developed it to join two rotating components reliably in 1864 and got a patent for the same. Morse started a Morse Twist Drill and Machine company in the same year with an investment of $30,000 from the stockholders.
Like all relationships, things didn’t stay smooth for long—Stephen Morse had a fallout with the company board and ended up resigning just four years after starting the company. There’s not much info about what he did after that, but his legacy definitely lived on. The company grew into a giant in machine tool manufacturing, earning international fame.
However, it took a whopping 110 years for Morse’s brilliant idea to find its way into total hip replacements. And that too, only when ceramic heads came into play. Before that, monoblock metal implants were the norm, so there wasn’t even a need for a fancy coupling mechanism like the Morse taper.
One can think then “how did they fix the ceramic head on the stem” before Morse taper was inducted… yeah, they used to do it with glue or screw, the carpenter inside seems to be always at work! Prof. Mittlemeier, in 1974, was the first one to adapt Morse taper which unsurprisingly reduced the fractures of the head. Further developments were done Daniel Blanquaert in association with Ceraver in 1977. Even now, the reliable impacted fit we get between the trunion (male portion) and the bore (female portion) in our total hip prosthesis is the result of one man trying to make using machine tools easier a century and a half ago.
SuperPATH - #SurgicalPearl:
People are now moving from minimally invasive approaches to micro-invasive approaches for THA. SuperPATH is one such approach and is super interesting.
Supercapsular percutaneously assisted total hip (SuperPath) approach is a direct superior portal-assisted approach to total hip arthroplasty (THA) that utilizes the interval between the gluteus minimus and the piriformis to access the hip. The major steps of this procedure:
The patient is in the standard lateral decubitus position with the involved leg in the“home position,” that is,45° to 60° of flexion, 20° to 30° of internal rotation, and slight adduction elevating the foot on a padded Mayo stand.
Exposure - Incision is from the tip of the GT 6 to 8 cm proximally in line with the femur in the home position, the gluteus maximus muscle is split by blunt dissection in line with the fibres, and the gluteus medius and minimus are retracted anteriorly, and the piriformis tendon is retracted posteriorly to access to the capsule.
Capsule is incised along the path of the skin incision from the saddle of the femoral neck to 1 cm proximal to the acetabular rim.
Femoral preparation - A channel is created in the superior aspect of the femoral neck from the femoral canal to the centre of the femoral head, using reamers, a round osteotome, and a curet.
Femoral broaching - Sequential femoral broaches are then used to complete the preparation and size of the proximal femoral canal while the head and neck remain intact.
Neck resection - The femoral neck osteotomy is performed level with the broach neck, and Schanz pins are used to rupture the ligamentum teres and remove the femoral head.
Acetabular preparation and placement - Acetabular preparation and cup impaction are done through a portal without needing the release of the iliotibial band or remaining external rotators.
Trial reduction - Trial reduction is completed using a bone hook and a T-handle to gently manipulate the femur.
Final implant assembly - Liner impaction is completed through the portal, and the remaining components are implanted.
Difficulty in following the technique? Check out the video here.
The Holy Grail for hip surgeries? #MostCited:
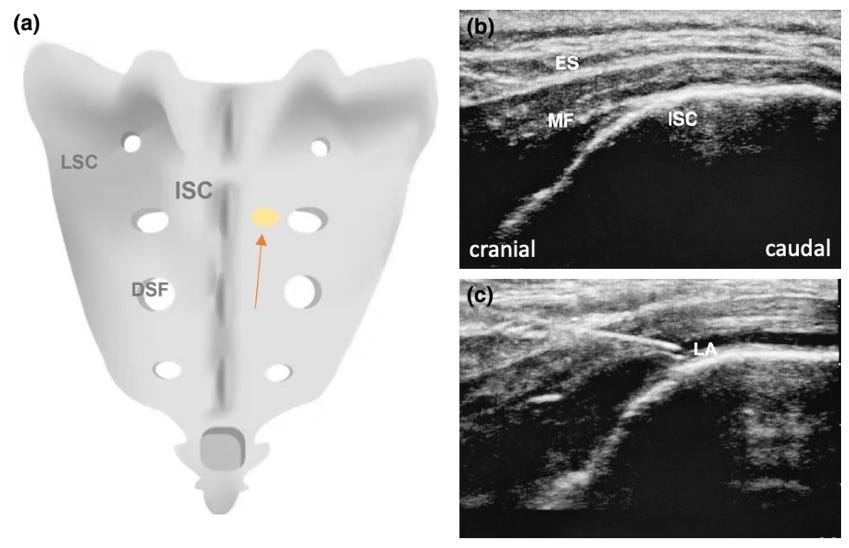
Spinal anaesthesia is a concern in elderly with multiple comorbidities. It is not always risk free. Sacral erector spinae plane block is now potentially considered as an alternative to conventional anaesthetic approaches in frail individuals with significant cardiovascular and respiratory comorbidity in procedures such as intramedullary nailing for proximal femoral fractures. A unilateral injection of local anaesthetic at the intermediate crest of the second sacral vertebra resulted in bilateral sensory block of the T12 to S2 dermatomes. The technique did not result in hypotension or motor block of the limbs, and the surgery was completed uneventfully.
Though this technique warrants further investigation to be considered as an alternative to spinal and general anaesthesia for hip and lower limb surgery, it now the hot cake over the table on New Year for the frail individuals sustaining hip fractures.
Shoulder I change my approach? - #InTrials:
A study by Roberts et al. compared the Direct Anterior Approach (DAA) and Mini-Posterior Approach (MPA) for total hip replacements, and the results are pretty much neck and neck. Early on, DAA showed slightly quicker recovery, but by a few weeks in, those perks were gone, and both approaches performed about the same. Fast forward 7.5 years, and there’s still no big difference between the two in terms of function, X-rays, or overall quality of life.
The scores for things like hip health (Harris Hip Scores, SF-12, HOOS) were super similar, and none of the numbers hit the “wow, that’s a huge improvement” mark. Complications? DAA had 4, MPA had 6—stuff like dislocations, wound problems, and a couple of rare re-dos.
Bottom line: Both approaches are solid for hip replacements. Surgeons can choose whichever method works best for their vibe and the patient’s needs, knowing the long-term outcomes are basically the same.

Answer to previous month question:

Spinous process osteotomy seems to be the most effective technique according to the meta-analysis by Wu et al.
Question of the month:
Which approach to hemiarthroplasty after femoral neck fractures has minimal complications?
Posterior approach
Direct anterior approach
Direct lateral approach
Anterolateral approach
Events to check out:
25th Annual Meeting of Arthroscopy Association of North America (AANA)
8 – 10 May 2025
Washington DC, United States
8 – 11 June 2025
Munich, Germany
28 – 31 May 2025 Rio-de-janeiro, Brazil
Cheers to a bright and beautiful year ahead guys
